Voice Disorder
Our voice is the sound produced in our throat that we use for speech or singing. Every person’s voice is unique to them in terms of its tone, loudness and pitch (highness or lowness). In order to produce voice, when we are speaking air moves from the lungs through two small structures in our throat, called the vocal folds. With the vocal folds closed, the air causes them to vibrate as it moves through them, resulting in a noisy sound or voice being produced. With the vocal folds open, air passes easily between them and we can produce quiet sounds with no voice, for example when whispering.
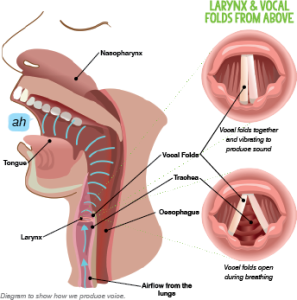
Diagram to show how we produce voice.
Everyone experiences a hoarse voice quality at times, for example after shouting and cheering too much for a favourite sports team or singing on a night out. These voice difficulties usually last for a short time with our voice then returning to normal.
A voice disorder occurs when the quality of the voice is abnormal for the individual, for a prolonged period. The term dysphonia is used when the voice presents with difficulties in terms of quality, loudness and pitch which are inappropriate for the speaker. The voice can sound the same or vary over time, ranging from a mild to severe difficulty. The term aphonia is used when someone completely loses their voice.
When children develop a hoarse or husky voice, it is usually during and/or after a cold or throat infection, which has caused inflammation of the throat and vocal folds. The voice is commonly back to normal within 2-3 weeks, but sometimes difficulties can last longer, and support is needed for the voice.
Causes of voice disorder
There are lots of different factors that can cause children to have voice disorders. If a child has a persistent difficulty with their voice, it is important that this is investigated to determine the cause(s), so that a suitable treatment can be identified. In very rare cases, a voice disorder indicates a more serious difficulty, so it is important that voice disorders are investigated fully.
In children, voice disorders are mainly due to vocal misuse, for example bouts of screaming, shouting and over-use of the voice. This can cause vocal fold nodules, often referred to as ‘screamer’s nodules’. When the vocal folds come together with too much force, for example when shouting, swelling can develop around the site of the collision. This can result in soft nodules developing, which often will recover within a few days of normal voice use. If the vocal misuse continues, the swelling can become more persistent and require treatment, with the child experiencing a voice disorder often characterised by hoarseness, discomfort and tiring of the voice.
Voice disorders can also be caused by physical or neurological difficulties, such as vocal fold paralysis, where one or both vocal folds is unable to move. 41% of children with velopharyngeal insufficiency (failure of the soft palate to close off the nose), such as children with Cleft Palate, have difficulties with voice quality. This is due to needing to push harder to maintain airflow through the mouth for speech, because of airflow being lost through the nose. Children with reflux can also experience difficulties with their voice, due to irritation and inflammation within the throat.
Less commonly, children can have voice disorders as a result of psychological difficulties.
Emotions are experienced both mentally and physically by our bodies, for example both excitement and anxiety have recognisable physical feelings in our bodies. Anxiety can result in increased muscle tension, which can affect the throat. Some children seem to be susceptible to expressing anger and frustration through tight and constricted voice use, which over time can result in a voice disorder. Children with Selective Mutism can develop a voice disorder, due to their significant speaking anxiety. For these children, the underlying cause of their voice disorder, speaking anxiety, would need to be supported first, with the likelihood that their voice disorder would then resolve.
Often a child’s voice disorder can be caused and/or maintained by multiple factors which impact on each other. For example, the difficulty could start due to vocal misuse resulting in poor voice quality, which could cause anxiety about communicating because of the sound of the child’s voice, resulting in further vocal tension.
Prevalence
The American Speech-Language-Hearing Association (ASHA) reports that the prevalence of voice disorders has ranged from 1.4% to 6% of the population. The most frequently diagnosed voice disorder in children is vocal fold nodules, which may be as high as 16.9% in school aged children. Voice disorders are significantly more common in males than females.
What to look for
Children with voice disorders may experience the following difficulties:
- Poor or variable voice quality, for example sounding rough or hoarse, breathy, weak, squeaky or having a tight, tense or squeezed quality
- Voice ‘breaks’ where the sound cuts out completely or is very slow to get going
- Difficulties with pitch, with the voice sounding too low or too high
- Difficulties with loudness, with the voice being too quiet or too loud
- Needing to use lots of effort when speaking and visible tension in the throat, neck and/or shoulders
- Poor quality or disappearing voice after long periods of use or at the end of the day
- Feeling of dryness or scratchiness in the throat
- Frequent coughing or throat clearing
- Reports of aching or pain in the throat when speaking
Myth Busting

Does shouting and screaming always cause voice disorders in children?
When working with children who have a voice disorder, it is often thought that you need them to stop shouting, screaming and singing altogether. All children shout, scream and sing and most do not develop a voice disorder, so it is not the actions themselves that are causing the difficulty, but the way they are being completed, e.g. excessively or with increased tension. It is important that children understand the factors that are affecting their voice and are reassured that they can scream and shout, but to try and do this in a healthier way.
Do we need to worry about a child’s ‘strange’ voice if they have always sounded like this?
For many children, their voice disorder will develop while they are at school and changes to their voice quality will be noticeable. Some children, however, are born with voice difficulties or will start school with poor patterns of using their voice already entrenched. Although they may have ‘always sounded like this’, if the child’s voice quality is inappropriate for their age, gender or culture it is important that this is investigated further.
Impact of voice disorder
The impact of voice disorder will vary from child to child and the severity of the disorder does not always directly correlate to the impact for the child. For example, a child may have a very mild voice disorder, but feel significant anxiety about the sound of their voice, resulting in it limiting their social life or activities. Voice disorder may impact on the following areas for children:
- Difficulty successfully communicating with adults and their peers
- Difficulty participating successfully in class discussion and group activities, for example if their voice quality results in them being difficult to understand within a noisy classroom
- Difficulty with social communication and interaction, as a result of not being understood or concerns about how their voice sounds
- Self-esteem and self-image difficulties as voice is very personal and reflects us as an individual. Voice disorder may draw attention to the child and result in teasing or bullying.
Strategies

The vocal folds are small, precious muscles which need to be looked after in order to maintain good voice quality. The following are recommendations for supporting healthy voice quality:
- Encourage the child to have good drinking habits. The vocal folds are covered in mucus, so it is important to keep them well hydrated. Dehydration can cause the vocal folds to be drier and work less effectively. Water is the best drink, as fizzy drinks or tea and coffee contain caffeine which can dry out the vocal folds. It is beneficial for children to have access to a water bottle at school, so that they can drink regularly.
- Encourage the child to try and avoid screaming, shouting or talking excessively loudly. Reward charts with visual representation of different volumes (e.g. using quiet and noisy animals), can be effective in supporting children to monitor their amount of talking or loudness.
- Encourage the child to avoid whispering for prolonged periods of time. Whispering pushes the vocal folds apart and causes increased strain.
- Reduce throat clearing or excessive coughing by encouraging the child to take a sip
of water. Repeated coughing and throat clearing bang the vocal folds together and will increase irritation and swelling. Blowing out air, sniffing and swallowing can all help the vocal folds to move apart and feel less tight and irritated. - Within the classroom, encourage pupils to put their hands up to answer questions instead of calling out, so that the child with voice disorder does not have to try and compete to
be heard. At home, it is important that the child does not have to shout or speak loudly to compete with siblings and that they are not shouting from different rooms to communicate with family members.
When should I refer?
As many children will experience hoarseness during their development or as a result of a cold or throat infection, not all children experiencing voice difficulties need to be referred for further support. If a child is experiencing difficulties with their voice quality that last longer than three weeks, it is recommended that you discuss your concerns with parents who can take the child to the GP to discuss this further.
For most children who are experiencing voice disorder, a referral to SaLT is recommended to determine causal factors and develop a suitable plan for treatment. Concerns about voice quality can be discussed with your local SaLT service. If children are experiencing persistent voice disorder or have voice difficulties that sound very abnormal, they would benefit from referral to Ear, Nose and Throat (ENT) or a Voice Clinic for specialist assessment of the voice, to determine what is causing the difficulty. In rare cases, the voice disorder may be the first symptom of something more serious, so it is important to get this investigated, even to rule this out. If a child has any difficulties with breathing, including noisy breathing at rest, or difficulties with swallowing, it is important that they are referred to ENT.
Role of SaLT
Most children with persistent voice disorder will need to be referred to SaLT for assessment, advice and support. The SaLT will complete an assessment of voice including a detailed case history to determine the causes of the voice disorder and enable a treatment plan to be made. Treatment for the child may include indirect work focused on modifying the environments where the child is communicating, including advice and strategies for parents. It may include work on vocal hygiene strategies, to support the child to understand the voice and factors that are affecting it, in order to change vocal misuse behaviours.
Some children may need direct therapy to change their vocal behaviours and help them to establish healthy voice production. In order to benefit from direct therapy, children need to understand many abstract concepts and have an awareness of their difficulties, so this is often only completed with older children, over the age of six. In order to make changes to voice, the child needs to complete practice and want to work on making their voice sound better. Some children are unconcerned or unaware of their voice disorder and for them it is likely that direct therapy will not be effective. As children grow, their vocal folds also grow and difficulties with voice may resolve on their own, but if not, treatment can always be carried out later when the child is motivated or old enough to understand the importance.
Further Information
British Voice Association (BVA) – www.britishvoiceassociation.org.uk
RCSLT Voice Overview – www.rcslt.org/speech-and-language-therapy/clinical-information/voice
Read more about supporting teachers’ voice in The Link magazine, issue 6
Please login to view this content
Login