Speech Sound Disorder
Speech is the physical production of sounds, which we combine to say words, phrases and sentences clearly. Children who have a speech sound disorder have gaps in their speech sound system, resulting in difficulty expressing themselves clearly. The production of speech is a very complex process involving moving the articulators (including the lips, tongue and palate) to alter the airflow through the mouth and nose, resulting in different sounds being produced.
Speech sound disorder is an overarching term used to describe children who have difficulties with speech production. There are a number of different systems for classifying speech sound disorders and there is currently no universal agreement about the best system to use. In this section we have outlined the subcategories of speech sound disorder commonly used by SaLTs when diagnosing children and describing their difficulties.
Speech development
When children are learning to talk, it is normal for them to make some predictable speech sound errors. These predictable errors are attempts to make the words easier to say as their mouth, nose and throat develops. For example, children might commonly say “tar” for ‘car’ or “wocket” for ‘rocket’.
The speech sounds develop in more or less the same order for most children, with some sounds being learned earlier (e.g. p, m), and some sounds being learned later (e.g. r, th). 0020At first, children only have a limited range of sounds that they can produce and as their fine motor, listening and monitoring skills develop, they are able to produce a wider range of sounds. It is therefore normal, for the first two years, for only people very close to the child to be able to fully understand their speech. These errors have usually stopped by the time a child is five years of age, with only occasional errors seen with words or sounds. Although there is variation between children, most children should be able to say the full range of English speech sounds by the time they are seven.
If a child is unable to produce sounds by the expected ages or has a pattern of speech errors that continues to be used, they may have a speech sound disorder.
| Age (Years; Months) | Established Sounds For 90% Of Children |
| 3;0 – 3;5 | p, b, t, d, k, g
m, n, ng f, v, s, z, h |
| 3;6 – 3;11 | w, l, y |
| 4;0 – 4;11 | ch, zh, j |
| 5;0 – 5;11 | sh |
| 6;0 – 6;11 | r |
| 7;0+ | th voiceless (think) and voiced (this) |
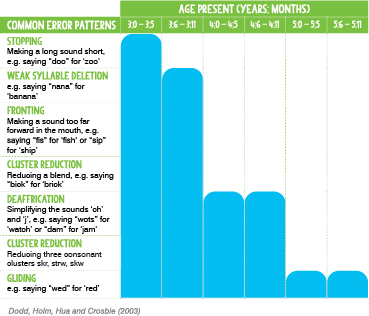
Common Error Patterns Graph: Dodd, Holm, Hua and Crosbie (2003)
Delay vs Disorder
When diagnosing children who have speech sound difficulties, a SaLT will look at the types of errors that the child is using. If a child is using speech error patterns which are observed in typically developing younger children, they would be described as having a speech delay. This means that their speech sound system is developing along typical lines, but at a slower rate. Children’s speech sound difficulties are more likely to resolve, if they have a delayed pattern of development.
If a child is presenting with speech error patterns which are not found in the speech of typically developing children, they are described as having a speech disorder. This means that their speech production is not following a typical pattern of development. Children are more likely to have persistent speech sound difficulties, if they have disordered error patterns. It is therefore important that children’s speech sounds are assessed to determine the types of errors that they are using. A child may commonly present with a mixture of delayed and disordered speech error patterns and in this case would be diagnosed with a speech disorder.
Why do some children have speech sound disorders?
Children can have speech sound disorders for a range of different reasons. Cleft palate, hearing impairment and motor disorders, such as Cerebral Palsy, can all result in physical difficulties producing sounds, but this only accounts for a small number of children.
For most children with speech sound disorder, there is no known or identifiable cause for their difficulties. Research has investigated some risk factors for developing speech sound disorder, which include gender (incidence is higher in boys than girls), family history of speech sound disorder and the presence of otitis media (middle ear infection). Some children have both speech sound disorder and language disorder, whereas some children just have speech sound disorder with no additional language difficulties.
Prevalence
Studies that have looked into the prevalence of speech sound disorders have reported rates ranging from 2.3% to 24.6% and the estimated prevalence rates vary greatly due to inconsistent use of classification systems for speech sound disorders. There is consensus that referrals decrease with age, with approximately 75% of children with speech difficulties in pre-school, having age appropriate speech by age six.
Myth Busting

Does working on non-speech oro-motor tasks improve speech?
It was previously thought that working on non-speech oro-motor movements with children would help to develop their speech sound skills, for example using programmes like Mr Tongue. It is now known that this is not effective as the specific movements required for producing speech sounds are very different from those used in non-speech movements. The exercises were also used to build up strength within the muscles, however as speech requires very fine and precise muscle movement coordination, building up strength will not improve speech production.
Does tongue tie cause speech sound disorders?
A child with tongue tie has a tight connecting strand from the floor of the mouth to the underside of the tongue. It is often thought that having a tongue tie will cause speech sound difficulties, however research indicates that there is no evidence suggesting a causative link between tongue tie and speech. A small number of babies need to have their tongue tie cut as it affects feeding. If the child can raise their tongue to the alveolar ridge (behind the top front teeth), they have sufficient movement to make all speech sounds.
Will children with speech difficulties just grow out of it?
Some children’s speech sound difficulties, particularly those with speech delay, may resolve over time without specific support. For many children, particularly those with more disordered speech error patterns, this is not the case and it is cause for concern if a child’s speech is still difficult to understand at age four. If speech sound disorder is not identified and support put in place, a child is at risk of persistent speech sound disorder during their school years, affecting literacy development, overall academic achievement and self-esteem. When children have language difficulties in addition to speech sound difficulties, their risk of persisting difficulties is higher.
Subtypes of Speech Sound Disorder
There is currently no universal agreement for classifying speech sound disorders, however therapists often use terms to describe the types of errors that a child is presenting with. These include articulation disorder, where a child has difficulty producing a sound in isolation, phonological disorder, where the child can say the sound in isolation but has difficulty producing it within the context of a word and Developmental Verbal Dyspraxia (DVD) where a child has difficulty with motor planning for speech.
It can be difficult to cleanly differentiate between articulation and phonological disorders, with some children having both types of speech sound errors, therefore many clinicians prefer to use the broader term speech sound disorder. A SaLT may refer to children having one or both types of these errors, which require different treatment approaches.
Children who are bilingual or multilingual are thought to have two or more separate sound stores, one for each language. This means that they may make different speech sound errors in each language. If the child has an articulation disorder, these errors would be found in both or all of the child’s languages as it is a difficulty producing a specific sound or sounds. If the child has a phonological disorder, different sounds may be affected in different languages, as it is word and, therefore, language specific.
Articulation Disorder
Children who have an articulation disorder have difficulty physically producing a sound or sounds in isolation. Although this type of error is likely to happen in children with structural or neurological difficulties, such as Cerebral Palsy or cleft palate, most children who have an articulation disorder do not have any physical or structural difficulties. These children have difficulty developing the ability to produce speech sounds in order to achieve clear speech. This results in articulation errors including distortions (producing a sound in an unfamiliar way) such as producing ‘s’ with a slushy quality, and substitutions (replacing one sound with another) such as saying “thoap” for ‘soap’.
Phonological Disorder
Rather than difficulties producing individual sounds, children who have a phonological disorder make predictable, rule-based errors that affect more than one sound. These errors may include consonant deletion, fronting (moving sounds made at the back of the mouth to the front of the mouth) and stopping (saying longer sounds as short sounds). The child has systemic problems relating to different sound groups, rather than individual sounds. Errors typically include omissions (the whole sound is left out of a word completely) such as saying “bo” for ‘boat’, or substitutions (replacing one sound with another), such as saying “d” for ‘s’, e.g. “dun” for ‘sun’ and “bud” for ‘bus’. This results in the child having a restricted system for making contrasts between different words, resulting in reduced intelligibility.
Phonological Disorder is broken down into two types; Consistent Phonological Disorder and Inconsistent Phonological Disorder. In Consistent Phonological Disorder the child makes the same error every time they say a sound or word, so their production of words does not vary. Their sound system is predictable and the specific error patterns they are using can be worked on in treatment. In Inconsistent Phonological Disorder the child makes different errors when attempting to say words, for 40% or more of the words attempted. Their sound system is unpredictable, and treatment needs to initially focus on developing their ability to produce words more consistently each time.
Developmental Verbal Dyspraxia (DVD)
Developmental Verbal Dyspraxia (DVD), also known as Childhood Apraxia of Speech (CAS), is a subtype of speech sound disorder, resulting from an impairment in motor planning and programming. Children with DVD have difficulty in making and coordinating the precise movements required for speech production, even though there is no damage or weakness to their muscles or nerves. They have difficulty with the speed, accuracy and timing of the movements needed to produce clear speech.
In order to produce speech sounds, messages travel from the brain to the mouth, telling the muscles how and when to move. For children with DVD, the messages do not get through correctly, resulting in the child not being able to move their lips, tongue, jaw and palate in the right ways. This results in difficulty planning and coordinating the precise movement of muscles to produce individual speech sounds and to sequence sounds together into words and sentences.
Children who have DVD are often unintelligible, even for family members, as this is a significant speech sound disorder. DVD makes a child’s speech sound unusual, not just like a younger typically developing child. At around 3 years old, a child with DVD may have a very limited spoken output and may be thought to have language difficulties. Then as the child’s vocabulary increases, it becomes more obvious that they are only able to produce a limited number of sounds in words. As children with DVD get older or make progress, the difficulties they have can change and their speech can sound different.
The causes of DVD are not fully understood and often cannot be identified, but there is evidence to suggest that DVD may be inherited for some children. Some children with DVD also have oro-motor dyspraxia, affecting their ability to make and coordinate non-speech movements of the lips, tongue, palate and throat. Many children with DVD also have Developmental Coordination Disorder (DCD) affecting control over gross and fine motor body movements.
Prevalence
It is agreed that DVD exists as a distinct subtype of speech sound disorder, but due to lack of a consistent definition and identification of children, it is difficult to determine the prevalence of the disorder. Research does indicate that the condition is rare.
Difficulties
There is no specific definition or agreed set of diagnostic characteristics for DVD, but there is general agreement about the types of difficulties that children with DVD commonly have. A child would receive a diagnosis from a SaLT if they presented with a cluster of agreed symptoms or ‘features’. Children are often given a diagnosis of ‘features of DVD’. The features or areas of difficulty can range in severity from mild to severe and have an increasing impact on children as the demands of communication increase. As DVD is a rare speech sound disorder, and the presentation can change over time, it is recommended that children are diagnosed and supported by a specialist SaLT who specialises in speech sound disorder and/or DVD.
Children with DVD will present with a range of difficulties or ‘features’, which will change over time, and may include:
- A limited range of consonant and vowel speech sounds
- Difficulty making sounds or repeating sequences of sounds or words
- Overuse of one sound, often known as a favoured articulation, for example saying “hoo” for ‘shoe’, ‘blue’ and ‘do’
- Inconsistent errors on sounds in repeated productions of syllables or words
- Lengthened or disrupted transitions between sounds and syllables, with difficulty sequencing sounds correctly within syllables and words
- Using inappropriate prosody, affecting rate of speech, rhythm, stress and intonation, e.g. some children may speak in a monotone placing equal stress on each syllable in words or have an odd sounding intonation with stress placed on unusual words in sentences
- Voice difficulties, affecting volume, pitch (highness or lowness) and quality of the voice
- Making groping or searching movements with their lips and tongue when trying to say a sound or word
- Difficulty with feeding, sucking and chewing in early infancy
Top Tip

When working on speech sounds, it’s important to ignore the spelling of words and focus on the sounds, e.g. the word shoe has two sounds ‘sh’ and ‘oo’. It is better to use pictures and sound cards, as using the written word when working on speech sounds can confuse children.
Impact of speech sound disorders
In addition to being unable to communicate successfully when speaking, having a persistent speech sound disorder, can impact on a range of different areas for pupils:
- Difficulty accessing education and, in particular, developing literacy skills
- Increased risk of mental health difficulties, including low self-esteem, lack of confidence and an increased risk of bullying
- Emotional and behavioural difficulties, which can develop as a result of frustration or anxiety
- Difficulty forming relationships and experiencing social isolation
- Increased risk of school exclusion, involvement with the criminal justice system and reduced opportunities for employment
Children with a diagnosis of ‘features of DVD’ are at an increased risk of early
and persistent difficulties with speech, expressive language and literacy. If children have poor intelligibility when they start school and have DLD or language disorder, in addition to their speech disorder, they are at greater risk of poor academic and social outcomes.
Strategies

- If you don’t understand what a child is trying to say, help them to find other ways of telling you, for example taking you to it, encouraging them to draw, thinking of other words they can use or giving them alternatives, e.g. ‘Do you want a pen or pencil?’
- Using a home-school contact book can be very beneficial to share information about what the child has been doing at home or any important news, so that you have an idea of what the child might want to tell you about. The contact book can be used to find out the names of family, friends and pets, so that you have a better understanding of words the child might be frequently using. It can also be used to write in information about what the child has done during the day at school, so that parents can use this to better understand what the child might want to tell them about.
- Once you have understood what the child has said, repeat back the child’s utterance to show them that they have successfully conveyed their message, e.g. if the child says “bid fis”, you say ‘Yes, a big fish’.
- Avoid asking the child to repeat what they are saying too many times. Not only will this increase their frustration and possibly reduce their motivation to attempt to communicate, it will reinforce the incorrect speech error pattern in their word store.
- Use visual support, such as Cued Articulation, which gives the child a visual cue for each sound, including its placement and the type of sound that it is. Focus on sounds that the child is working on currently or struggling with, to emphasise these in your own speech.
- Rather than asking children to slow down their rate of speech, slow down your own rate of speaking. This will mean that they are more likely to use a slower rate themselves and will give them additional time to process information and formulate what they want to say.
When working with a child on their speech sound production
- Make activities fun, as this will ensure that the muscles are relaxed, and the child will be more motivated to complete activities.
- Even if the child doesn’t achieve the sound you were aiming for, give them lots of praise for effort, e.g. ‘Good try, I can see you were thinking really hard about making that sound.’
- Progress in changing habitual patterns of speech sound errors can be slow, so it is important to be patient and encourage the child to keep trying.
- Aim to have lots of repetitions of a sound in each session, for example practising saying the sound ten times in a row at whichever level you’re working at (isolation, short words, longer words, sentences).
- If the child makes an error, stop them and encourage them to correct this before continuing with the drills, as repeatedly saying the sound incorrectly will reinforce the error pattern.
- Once the child is able to produce the sound in isolation, words and sentences, give them reminders to use their new sound in their general talking. Encourage them to try and ‘fix up’ any errors themselves by asking graded prompt questions; ‘Is it fis or fish?’ Then ‘Is it fis?’ Then ‘Did that sound right to you?’ to develop their ability to self-correct any errors and monitor their talking.
- If the child is unable to achieve a sound or activity over lots of tries, it is recommended that you stop working on that task. The failure is likely to make the child feel more negative about their speech and less motivated to continue working. Choose another sound or activity to work on and then go back to the task at a later time. Limited progress with speech sounds may indicate that further support is needed from SaLT, such as a detailed assessment and intervention plan.
Top Tip
Send home pictures and activities for parents to practise with them. The more practice the child completes the more quickly they are going to make progress. It is important to share strategies and techniques that work for the child with all adults communicating with them.
Supporting literacy development in children with speech sound disorders
Children with speech sound disorders often struggle to successfully develop literacy skills. Children with severe phonological disorder and DVD experience severe and persistent literacy impairment due to difficulties with phonological awareness. Children with DVD have significant difficulty producing individual sounds and even more difficulty blending the sounds together, even if they are able to read a word. This, therefore, significantly affects the children’s academic attainment as reading, writing and spelling are involved in every aspect of school.
The typical strategy used when learning a new word is to rehearse it verbally, until it is stored in our word bank. For children with speech sound disorders, the word will be produced incorrectly when rehearsed verbally or said a different way each time it is spoken. This means that there will be an incorrect or incomplete sound sequence stored in relation to that word. Then each time the child says, reads or spells that word in the future, they will use the incorrect or incomplete sequence stored, reinforcing the speech sound error. Solely teaching phonics is, therefore, not a useful way for children with speech sound disorders to learn to read and spell, as they are unable to produce sounds and words clearly.
It is important that phonics teaching is combined with other approaches to ensure the best opportunities for children with speech sound disorders to learn to read and spell:
- Make learning to read words a receptive task, asking the child to find the word from an adult or peer’s production, rather than needing to read the word out loud themselves, which they would be unable to do correctly
- Use multi-sensory approaches when learning new words including signs, cued articulation and visuals to support the written word
- Teach specific reading and spelling rules, e.g. frequent spelling patterns. Use colour coding systems as a visual reminder for sound groups and spelling patterns
- Continue to teach phonics, but build in time for repetition and revision as progress will be slower with pupils with speech sound disorder
When to refer
Children with speech sound disorders need support in order to make progress with their speech sounds, spoken language and learning, particularly children with persistent speech sound disorder. Completing a Speech Link assessment screening of any children that you have concerns about will determine which children can be supported by a programme of activities in school and which children need to be referred to SaLT for further assessment and advice. Children who are identified should be referred to SaLT as soon as possible and you should discuss with them any children who you have concerns about.
One of the strongest predictors of persistent speech sound disorder has been found to be intelligibility; children whose mothers reported that they were unintelligible to unfamiliar adults at age three, were 140% more likely to have persistent speech sound disorder at age 8. Any child that is unintelligible at age three, should be referred to SaLT. Using an intelligibility rating scale, such as the one included in the Speech Link package, can help to identify children who are at risk of developing a persistent speech sound disorder and, therefore, need to be referred to SaLT.
Children who are difficult to understand at school entry or who have speech difficulties that persist beyond the age of five and a half are also at risk for persisting speech sound disorder and should be discussed with the SaLT service. If the child has both speech sound and language difficulties, their risk is increased.
Children with ‘features of DVD’ are usually already identified because of their severe speech sound disorder, however there is a range of severity levels and because their difficulties change over time, less severe presentations may not be identified until the child is at school.
Role of SaLT
Most children with speech sound disorder need assessment and direct intervention from a SaLT in order to make progress. The impact of a speech sound disorder can be very significant in terms of the child’s ability to interact and communicate successfully, so it is important that support is put in place as soon as possible.
Once a referral has been completed, the SaLT will complete an assessment to determine the types of errors a child is making, to diagnose whether they are presenting with speech delay or speech disorder, and then the type of speech sound disorder they have. This will determine the most appropriate intervention for the child. For children with speech delay, the most appropriate course of action may be to give them some time for these difficulties to resolve. For children with speech sound disorder, a programme of activities carried out by school may be the most appropriate intervention or children may require direct intervention from a SaLT. This would need to be determined following assessment by SaLT. If a child is receiving direct therapy sessions, it is important that parents and school staff attend, at least some of, these sessions for demonstration of activities and strategies, so that follow up work can be completed at home and at school.
It is recommended that children with DVD are supported by a specialist SaLT in speech sound disorder and/or DVD. They require a specific intervention programme, with regular follow up work completed by parents and school staff. Without support, children with DVD will not make progress.
Some children have significant speech sound disorder that means it is difficult for them to functionally communicate their wants and needs, even to familiar adults. These children may need Augmentative and Alternative Communication (AAC) to provide an alternative means of communicating whilst they are working on developing their speech sound skills. This may include different ways of communicating such as using signing, pictures and symbols or specialist equipment that can be programmed to be their voice. Most children make progress with their speech sounds through intervention, however in some cases, children are unable to make enough progress to achieve intelligible speech and they may need to continue to use AAC to have a functional communication system.
Children need to have a level of motivation to work on their speech sound skills, as regular practice is required to make changes to established error patterns. It is important that activities are made fun and for older children the importance of the therapy sessions should be explained, as the child’s motivation to complete activities can be a big factor affecting their progress. This needs to be taken into account when planning support and for some children, who are not motivated to work on their difficulties, therapy may need to be delayed until they are older.
Children who have DLD or language disorder in addition to speech sound disorder, may need support to develop their language skills first, for example to ensure that they can understand and use a range of words, before they can work on developing their speech sound skills.
Further Information
Dr Caroline Bowen Speech-Language Therapy – www.speech-language-therapy.com
RCSLT Overview of speech sound disorders – www.rcslt.org/speech-and-language-therapy/clinical-information/speech-sound-disorders
For information about DVD and DCD visit:
Dyspraxia Foundation – www.dyspraxiafoundation.org.uk
Read more about Phonological Awareness in The Link magazine, issue 1; DVD in The Link magazine, issue 4; and Speech Delay vs Speech Disorder in The Link magazine, issue 5.
Please login to view this content
Login